













Understanding Heart Valve Anatomy: How Many Valves in the Heart?
Dr. Hriday Kumar Chopra
Textbooks often start with chambers and arteries, yet the quiet arbiters of flow decide cardiac efficiency. I mean the valves. A simple question drives clarity here: how many valves in the heart. The answer frames everything about circulation, pressure, and rhythm. In this explainer, I set out a precise tour of structure and motion, then highlight what fails, why it matters, and what I would prioritise in practice. Clean mechanics first, clinical nuance second.
The Four Heart Valves
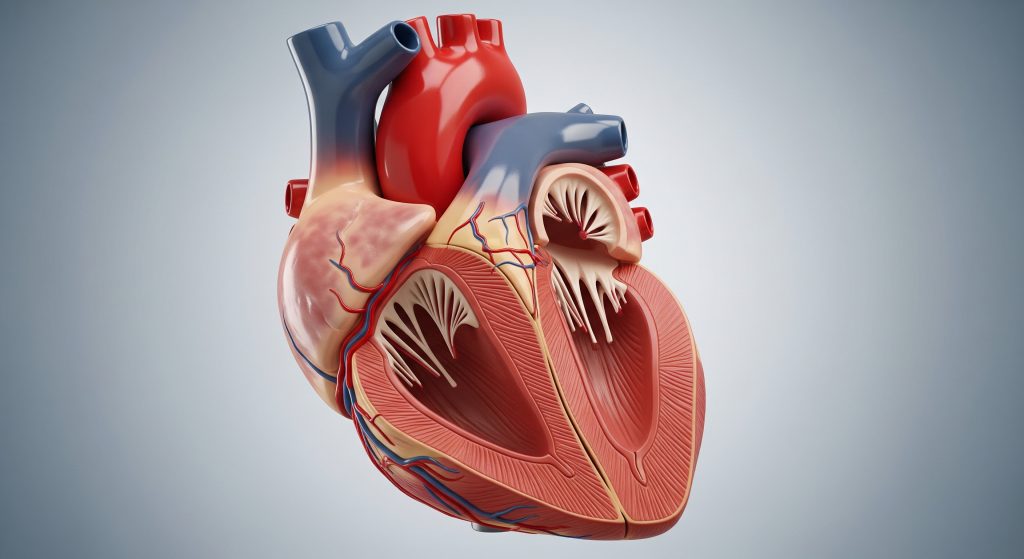
Clinically, the answer to how many valves in the heart is simple: four. Their architecture is compact, their timing exquisite, and their reliability remarkable under lifelong load.
|
Valve |
Primary role |
|---|---|
|
Tricuspid |
Controls right atrium to right ventricle inflow |
|
Pulmonary |
Regulates right ventricle outflow to pulmonary artery |
|
Mitral |
Directs left atrium to left ventricle inflow |
|
Aortic |
Governs left ventricle outflow to the aorta |
1. Tricuspid Valve
I view the tricuspid as the right heart’s gatekeeper. It has three leaflets anchored by chordae tendineae and papillary muscles. It opens during right ventricular relaxation, then seals to prevent regurgitation during contraction. Subtle leaflet thickening can raise venous pressure and cause ankle oedema. A simple example is functional tricuspid regurgitation in long‑standing pulmonary hypertension.
2. Pulmonary Valve
This semilunar valve sits at the exit of the right ventricle. Its three cusps open with systolic ejection and snap shut when pulmonary artery pressure exceeds ventricular pressure. Congenital stenosis narrows this outlet and elevates right ventricular workload. In adults, endocarditis or prior interventions may distort cusp coaptation, leading to diastolic backflow.
3. Mitral Valve
The mitral has two leaflets, a generous orifice, and a complex subvalvular apparatus. Precision of coaptation matters because pressures on the left are higher. Degenerative prolapse causes mid‑systolic displacement and a late systolic murmur. Rheumatic involvement thickens leaflets and fuses commissures, restricting inflow and raising left atrial pressure.
4. Aortic Valve
Engineering elegance meets durability here. Three semilunar cusps open under high pressure, then close to protect the coronary ostia and maintain diastolic pressure. Calcific aortic stenosis arrives insidiously and reduces valve area. The ventricle compensates with hypertrophy, then decompensates. Regurgitation, by contrast, loads the ventricle with volume every diastole.
Heart Valve Function and Blood Flow
How Heart Valves Work
I think in terms of pressure gradients and laminar flow. Valves open when upstream pressure exceeds downstream pressure and close when that gradient reverses. Leaflet geometry, chordal tension, and annular shape maintain a tight seal. This is the essence of heart valve function. It also clarifies how many valves in the heart coordinate to create one continuous circuit.
Blood Flow Through the Valves
Flow follows a fixed path: systemic veins to right atrium through tricuspid into right ventricle, then across the pulmonary valve to lungs. Oxygenated blood returns to left atrium, crosses the mitral into left ventricle, then ejects through the aortic valve to the body. Four valves. One loop. This is how many valves in the heart work in sequence without collision.
Common Heart Valve Problems
-
Stenosis: narrowing that obstructs forward flow and raises upstream pressure.
-
Regurgitation: incomplete closure that allows backward flow and volume overload.
-
Mixed disease: combined narrowing and leakage with complex haemodynamics.
Symptoms cluster around breathlessness, fatigue, reduced exercise tolerance, and oedema. Timing is critical because chambers remodel under stress. Decisions hinge on severity, mechanism, and surgical risk. This is where knowing how many valves in the heart and their interdependence prevents tunnel vision.
Understanding Your Heart’s Four Valves
When patients ask for a single takeaway, I emphasise synchrony. Each valve protects the next chamber, and the next circuit. A structured summary helps: the tricuspid and mitral admit blood during ventricular relaxation, while the pulmonary and aortic control ejection. That interplay defines heart valve function. It also explains why small structural changes can have outsized effects.
Frequently Asked Questions
Which heart valve is most important?
Clinically, the aortic valve usually carries the highest consequence because left ventricular outflow drives systemic perfusion. That said, context matters. Severe mitral disease can be equally disabling.
Can you live with damaged heart valves?
Yes, to an extent. Many people remain stable with monitoring and medication. When thresholds are crossed, timely repair or replacement restores forward flow and protects ventricular function.
What happens when heart valves do not work properly?
Stenosis raises pressure upstream and strains the chamber. Regurgitation causes volume overload and dilation. Left untreated, these changes impair output and raise heart failure risk.
Are heart valves the same in all people?
Anatomy is broadly consistent, but there are variants. Bicuspid aortic valve is a common congenital difference. It affects durability and surveillance plans over the long term.
How do doctors check heart valve function?
I rely on echocardiography first. It quantifies gradients, regurgitant volume, and chamber response. Cardiac MRI and catheterisation support complex cases or pre‑procedure planning.